What We Do
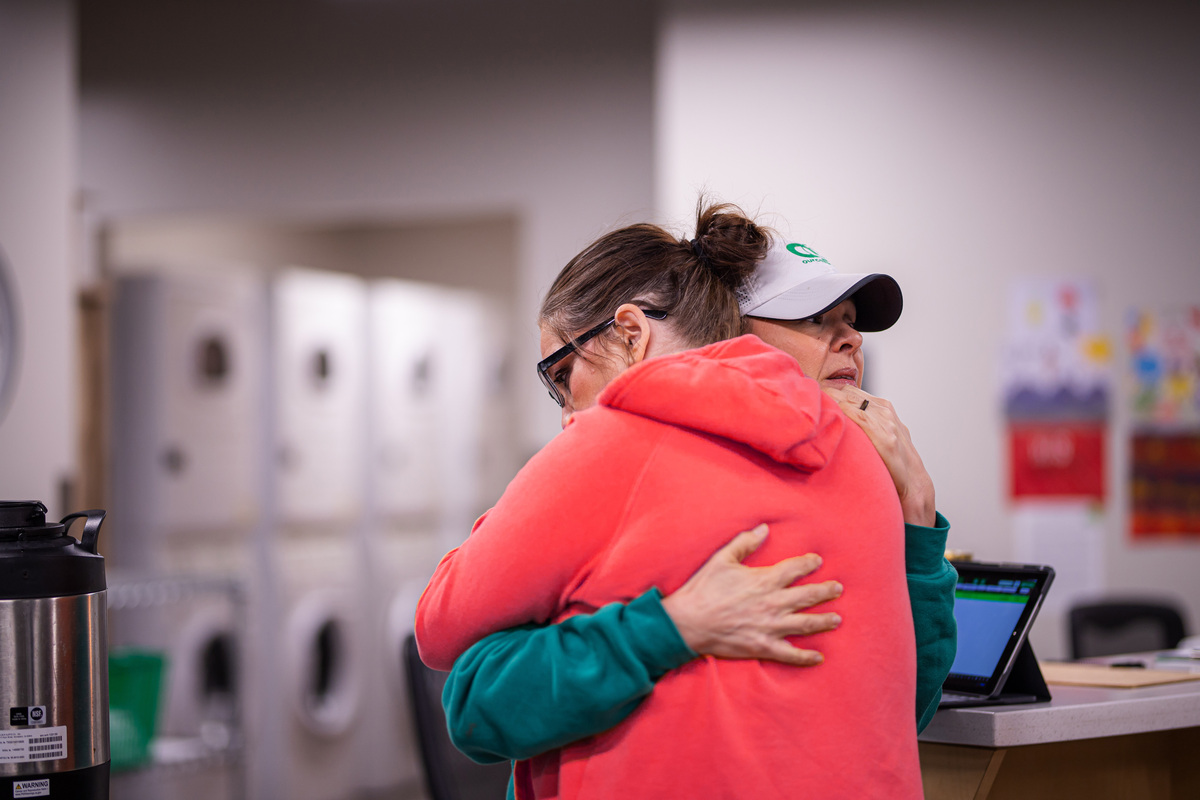
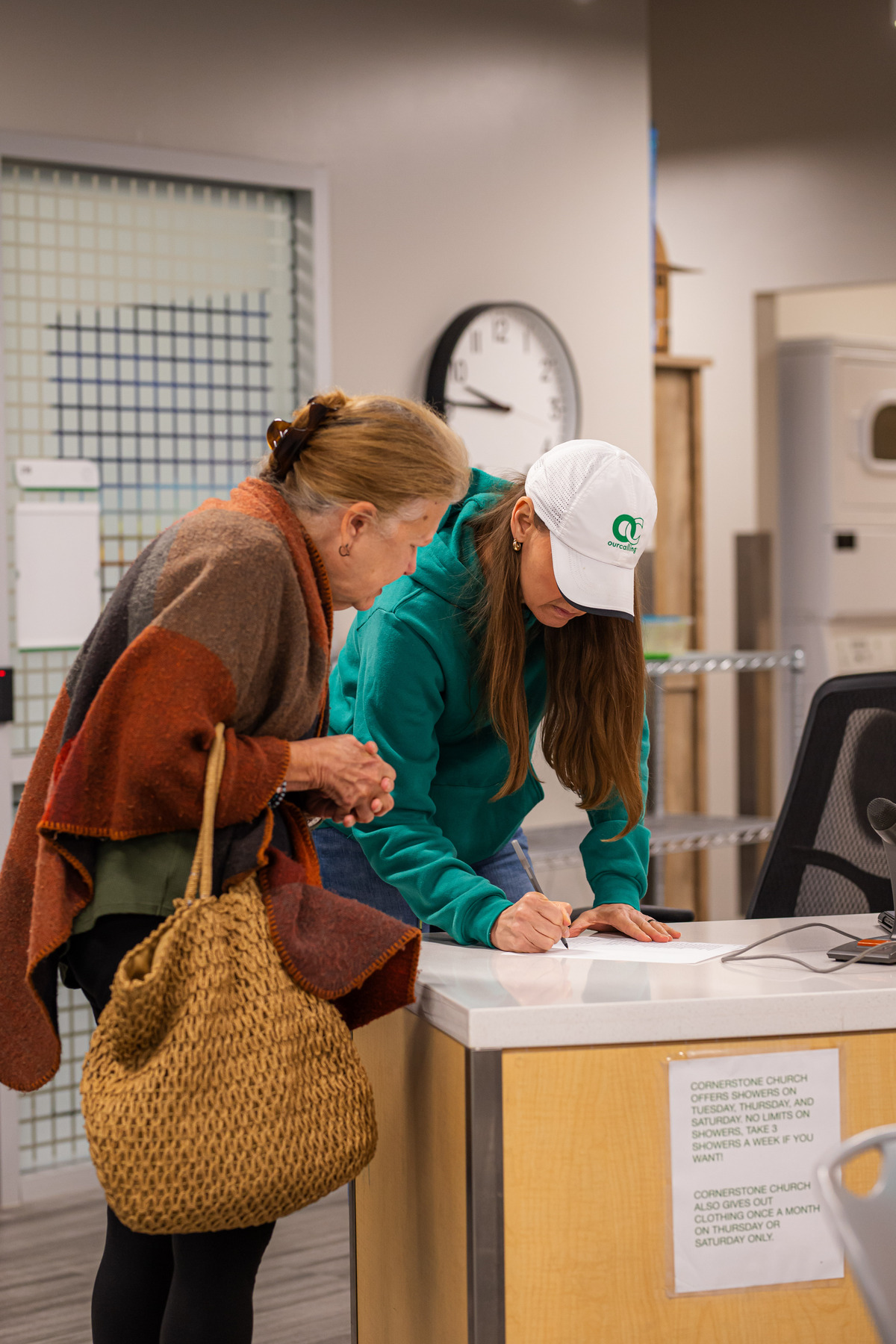
OurCalling helps our unsheltered homeless neighbors walk with Jesus and get off the streets. Everyday we ask two questions: “Will you trust the Lord?” and “Can we help you off the streets?”
Everything we do at OurCalling is rooted in our “3 C’s”
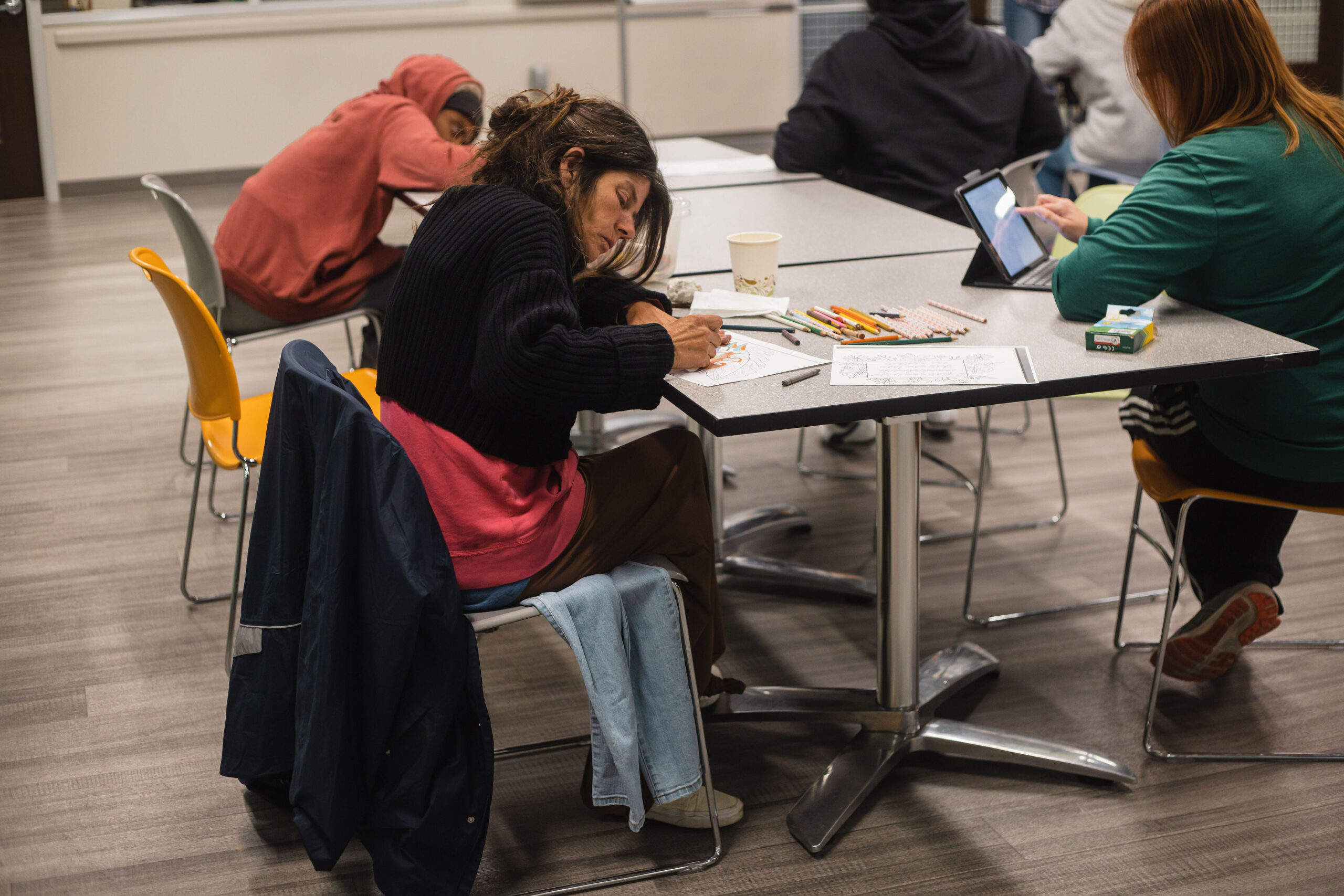
Understanding Homelessness in Dallas
10,000
+
men, women, and children are experiencing homelessness in Dallas
80
%
of them are unsheltered and have to sleep outside, in their cars, and under bridges every night
32
%
of people experiencing homelessness are women
72
people become homeless in Dallas each week

















2023
Impact
1359
Exits from Homelessness
94
K
Resources Distributed
140
K
Meals Served
2854